

Your first employment agreement isn't a fixed offer; it's a clinical revenue proposal that requires an objective economic response. You've spent years mastering complex pathologies, yet the transition to attending often feels like entering a boardroom without a map. It's common to feel a sense of unease when presented with a "standard contract" that seems to overlook your specific revenue-generating potential. Because physician contract negotiation for residents is rarely taught in medical school, many new attendings enter the workforce without realizing that the average physician salary has reached approximately $386,000 in 2026.
You shouldn't have to guess your worth or rely on outdated anecdotes. This guide will show you how to leverage specialty-specific economic value data to secure a contract that reflects your true market value. You'll learn to interpret technical terms like tail coverage and wRVUs with the same precision you apply to a clinical diagnosis. We'll provide a clear framework for a negotiation rooted in economic reality, ensuring you transition from residency with the confidence that comes from rigorous analysis.
Key Takeaways
- Understand why the transition to attending status represents your peak window of leverage and why the "standard contract" label is often a tactic used to limit your negotiation power.
- Move beyond the limitations of the wRVU model by quantifying your total Physician Economic Value, which accounts for the actual revenue you generate for a healthcare system.
- Learn to utilize objective benchmarks from CMS and RAND pricing to strengthen your physician contract negotiation for residents, moving past the biases found in traditional, self-reported salary surveys.
- Identify the critical components of a data-backed negotiation, from securing adequate tail coverage to ensuring your base compensation aligns with current market realities.
- Discover how a Specialty-Specific Revenue Analysis can translate your expected clinical workload into a clear benchmark for informed professional conversations.
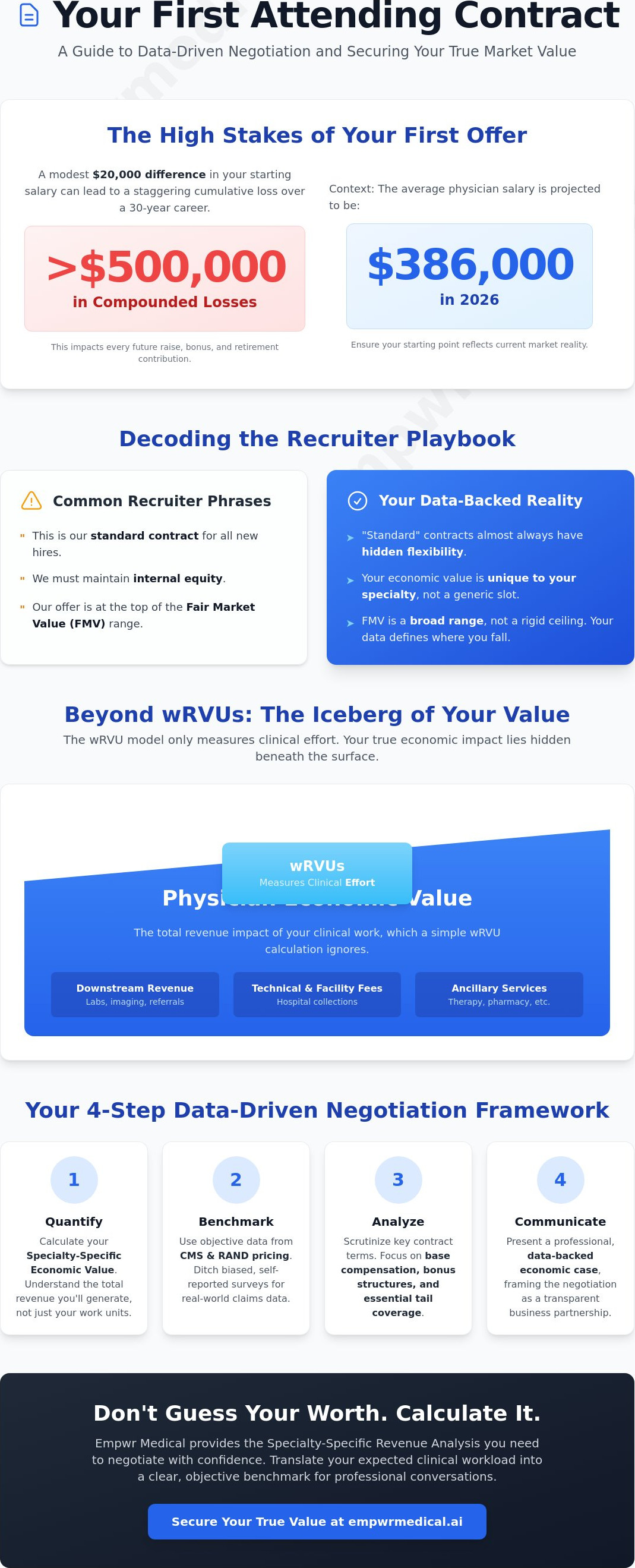
The High Stakes of Your First Attending Contract
The transition from a PGY-3 or PGY-4 resident to a full-time attending physician represents the most significant window of professional leverage in your career. At this juncture, you're no longer a trainee in a subsidized position; you're a high-value clinical asset capable of generating substantial revenue for a healthcare system. Many residents approach this transition with a mindset of gratitude rather than one of strategic partnership. This often leads to the passive acceptance of the first offer presented, a move that can have staggering financial consequences. A $20,000 difference in starting salary, when compounded by annual percentage raises and retirement contributions over a 30-year career, can result in a cumulative loss exceeding $500,000. The math is simple. The stakes are high.
Effective physician contract negotiation for residents begins with reframing the conversation. Negotiation isn't an adversarial act or a sign of being "difficult." Instead, it's a professional standard that demonstrates your understanding of the healthcare economy. Before signing, understanding the basics of an employment contract is essential to recognize how specific clauses affect your long-term autonomy and earning potential. You're establishing the foundation of your professional life.
Decoding the Recruiter Playbook
Recruiters often utilize a specific set of phrases designed to minimize a resident's perceived leverage. You'll likely hear that a document is a "standard contract" or that the organization must maintain "internal equity" among all new hires. These terms are frequently used to discourage individual adjustments. While health systems do use templates, there's almost always hidden flexibility within those frameworks. Recruiters often present Fair Market Value (FMV) as a rigid ceiling to cap compensation, but FMV is actually a broad range. Without your own revenue data, you're forced to accept their definition of "fair" rather than negotiating from a position of objective worth.
The Long-term Impact of Passive Acceptance
Your first contract sets the baseline for every future raise, bonus structure, and contract renewal. If you start at a lower benchmark, every subsequent percentage-based increase is calculated from that diminished floor. Beyond the financial metrics, there's a critical psychological shift that must occur. You're transitioning from a trainee to an independent economic contributor. Engaging in physician contract negotiation for residents establishes a precedent for professional advocacy. It signals to your employer that you're a data-driven professional who understands the value of your clinical output and expects a transparent, equitable partnership.
Beyond wRVUs: Understanding Your True Economic Value
While the previous section highlighted the high stakes of your initial agreement, the actual mechanics of your valuation often remain hidden behind a single metric: the Work Relative Value Unit (wRVU). Most medical residents are taught that wRVUs are the gold standard for measuring productivity. However, this model only tracks clinical effort; it doesn't quantify the actual profit you generate for a health system. To approach physician contract negotiation for residents with true authority, you must understand your Physician Economic Value. This represents the total revenue impact of your clinical work, including downstream revenue and technical fees that a simple wRVU calculation ignores.
The distinction between effort and economic value is where your leverage resides. A surgical specialist and a cognitive specialist might produce identical wRVU totals, yet their impact on the hospital's bottom line differs drastically based on facility fees and ancillary services. If you don't quantify this difference, you're essentially leaving your compensation to be determined by a system designed to maximize the hospital's "spread" rather than your professional worth. Understanding your specific revenue-generating potential is the first step toward a fair agreement.
The Limitations of the wRVU Model
The wRVU model is inherently limited because it fails to account for geographic adjustments or the specific payer mix of a practice. It treats every unit of work as a commodity. In reality, hospitals profit from the difference between what they pay you per wRVU and the actual collections they receive from insurers. As you prepare your strategy, consulting a comprehensive physician contract negotiation guide can help you identify these nuances. In 2026, the conversation is shifting toward transparency. With the CMS finalizing a 3.26% increase in the conversion factor for most physicians, the gap between what the system collects and what they offer residents is widening. You need to see the full picture to negotiate effectively.
Calculating Your Potential Contribution Margin
The Contribution Margin is the most critical number in your contract, yet it's rarely discussed with residents. This figure represents the revenue remaining after all variable costs associated with your clinical work are paid. It's the number the Chief Financial Officer (CFO) prioritizes. You can estimate your year-one impact by translating projected clinical volume into revenue using current CMS fee schedules. This proactive approach allows you to present a data-backed case before you see your first patient. Utilizing a Specialty-Specific Revenue Analysis provides the granular detail needed to demonstrate how your specific workflow contributes to the system's financial health, transforming a vague salary request into a precise economic proposal.
Leveraging Data: Salary Surveys vs. Real-World Revenue
Most candidates enter physician contract negotiation for residents relying on the same data points their employers use. This creates an immediate informational disadvantage. Traditional salary surveys, while common, often suffer from significant lagging. By the time a 2026 report is published, it typically reflects clinical activity and collections from 2024 or 2025. In a rapidly evolving healthcare economy, relying on these outdated benchmarks effectively anchors your career to yesterday's economic realities. You need real-time clarity to understand how current market shifts impact your specific valuation.
The gap between "Median Compensation" and "Economic Value" is where most residents lose potential earnings. A hospital's offer based on a survey median is designed to minimize their financial risk. It doesn't account for your specific revenue-generating potential or the unique market demand in your chosen geography. To negotiate effectively, you must shift from defensive comparisons to an offensive, data-backed strategy. This requires looking beyond what other physicians are paid and focusing on what payers are actually distributing to systems for your specific services.
The Flaws in Employer-Reported Data
Employer-reported data sets, such as those from the MGMA, can be influenced by the reporting entities themselves. Health systems have a vested interest in keeping reported averages low to maintain a manageable "Fair Market Value" ceiling. These surveys often fail to reflect the value of a high-volume specialist or the nuances of a specific payer mix. If you're entering a high-demand market, an "average" salary is actually a pay cut when adjusted for the revenue you'll generate. Moving toward independent, physician-led data sources is the only way to ensure the numbers you bring to the table haven't been filtered through an institutional lens.
Using RAND and CMS Data for Leverage
RAND pricing data provides a transparent look at what commercial insurers actually pay in your region, often revealing rates that are significantly higher than Medicare baselines. By utilizing the 2026 CMS fee schedule, which includes a 3.26% increase in the conversion factor for most physicians, you can build a bottom-up revenue model. This allows you to quantify your impact with clinical precision. Some industry professionals report that candidates who present these granular revenue estimates can secure offers that exceed initial proposals by double-digit percentages. Accessing a Physician Economic Value Platform allows you to perform these complex calculations without needing a degree in healthcare administration, providing the steady assurance of methodology during your final interview.
The Negotiation Framework: How to Present Your Case
Successful physician contract negotiation for residents isn't about being persuasive; it's about being prepared with objective evidence. Once you've identified your economic value, you must present it through a structured framework that shifts the conversation from personal needs to mutual ROI. This methodical approach ensures that you aren't just asking for more money, but rather proposing a fair exchange based on the clinical revenue you'll generate. The goal is to move the recruiter away from "standard" templates and toward a customized agreement that reflects your actual worth.
- Step 1: Conduct a pre-negotiation economic audit. Before the first meeting, use the Empwr Index to establish your baseline. This score benchmarks your professional worth against real-world revenue data.
- Step 2: Define your priorities. Distinguish between "Must-Haves," such as tail coverage and a base salary that reflects the 2026 average physician salary range of $386,000 to $458,257, and "Nice-to-Haves" like CME allowances or specific call schedules.
- Step 3: Frame the conversation around ROI. Position your compensation as a logical fraction of the total contribution margin you bring to the health system.
- Step 4: Handle rejection with tactical empathy. If a recruiter claims the offer is non-negotiable, use data-backed counters to highlight the gap between their proposal and the 3.26% increase in the 2026 CMS conversion factor.
Framing Your Value Proposition
A data-first opening sets the tone for a professional dialogue. Instead of stating what you want, start by introducing your findings. You might say, "Based on the specialty-specific revenue analysis for this region, my projected clinical volume aligns with a contribution margin of X." This shifts the focus from your personal desires to the operational reality of the practice. It's a template for success that positions you as a strategic partner. You're showing the employer exactly how your presence improves their bottom line, making it difficult for them to justify a lower offer.
Negotiating Non-Salary Terms
While base pay is vital, non-salary terms often provide the most significant long-term protection. Tail coverage is a critical "must-have" for residents transitioning to their first attending role. Negotiating for the employer to cover the cost of the "tail" on your malpractice policy can save you tens of thousands of dollars if you eventually leave the practice. Additionally, seek protected time for administrative or research duties to prevent burnout and ensure career longevity. Maximizing front-end cash through signing bonuses and student loan repayment is also standard in 2026. To ensure your case is bulletproof, you can generate your Empwr Index Report to lead your negotiation with the most accurate economic modeling available.
Empowering Your Career with Empwr Medical
The transition from medical training to professional practice is fundamentally a shift in responsibility. You're moving from managing patient outcomes to managing your professional equity. Successful physician contract negotiation for residents requires more than just a list of demands; it requires a sophisticated understanding of how your clinical labor translates into institutional revenue. Empwr Medical provides the analytical tools necessary to bridge the gap between clinical excellence and economic clarity. You've spent years mastering the science of medicine, and now it's time to master the economics of your own career.
Our Physician Economic Value Platform utilizes precise modeling to translate your projected clinical workload into objective revenue estimates. By inputting your expected patient volume and specialty-specific metrics, you can visualize the actual contribution margin you'll provide to an employer. This process removes the ambiguity often found in traditional negotiations. It's about using the same data-driven rigor you apply to a differential diagnosis to evaluate your first employment agreement. When you enter a room with quantified data, the conversation shifts from a request for better terms to a strategic discussion about professional value.
The Empwr Index Report for Residents
The Empwr Index Report for Residents serves as a definitive benchmark for your professional worth. It aggregates complex data points into a single, actionable score that you can bring to the negotiation table. This report levels the playing field by providing a Specialty-Specific Revenue Analysis that accounts for current market demand and geographic nuances. For a deeper look at how these metrics are derived, you can read about the Physician Economic Value Score: Quantifying Your Clinical Impact in 2026. Having this independent valuation ensures you aren't reliant on the employer's internal data, which is often optimized for their own financial interests. It gives you the steady assurance of methodology during high-stakes conversations.
Strategic Planning for Your First Year
Your first year as an attending is a critical period for establishing your long-term value. Data shouldn't just be used for the initial contract; it's a tool for ongoing strategic career management. By using our platform to track your actual clinical performance against your contract benchmarks, you can prepare for your first annual review before you even see your first patient. This proactive stance allows you to demonstrate your value with objective evidence, making future negotiations a continuation of a transparent, data-backed conversation. You're no longer just an employee; you're a strategic partner in the healthcare system. Claim your seat at the table by ensuring your professional worth is quantified and respected from day one.
Securing Your Professional Future with Economic Clarity
Entering the workforce as an attending physician is a pivotal moment that requires a transition from clinical training to strategic career management. You've seen how the "standard contract" is often a myth and why relying on lagging salary surveys can anchor your earnings to the past. By focusing on your true contribution margin and utilizing authoritative CMS and RAND data, you transform physician contract negotiation for residents into a data-backed proposal. This approach ensures your compensation reflects the actual revenue impact of your clinical work in 2026.
Empwr Medical is a physician-led platform designed to bring transparency to these high-stakes conversations. We provide specialty-specific and location-adjusted reporting to ensure your valuation is grounded in operational reality. You don't have to navigate this transition with uncertainty. Instead, lead with the quiet confidence that comes from rigorous economic modeling. Calculate your true economic value with the Empwr Index and start your career with the clarity you deserve. You've earned your place at the table; now ensure you have the data to stay there.
Frequently Asked Questions
When should a resident start negotiating their first attending contract?
You should begin the process approximately 12 to 18 months before your residency or fellowship concludes. This timeline provides the necessary runway to perform a specialty-specific revenue analysis and evaluate multiple offers without the pressure of an impending graduation date. Early preparation ensures you have sufficient time to leverage data and conduct informed conversations with potential employers.
What are the most common mistakes residents make in contract negotiations?
The most frequent error is accepting the "standard contract" myth without performing independent due diligence. Many residents focus exclusively on the base salary while ignoring critical non-salary terms like tail coverage or restrictive non-compete clauses. Failing to quantify your projected economic value often results in accepting an offer that sits well below your actual revenue-generating potential.
Are physician salaries truly non-negotiable at large academic centers?
No, salary rigidity at academic institutions is often an administrative preference rather than a fixed rule. While base pay scales may be more structured, other components like signing bonuses, protected research time, and relocation allowances remain flexible. Effective physician contract negotiation for residents in academic settings involves framing your requests around the specific clinical or research revenue you'll bring to the department.
What is tail coverage and why is it a major negotiation point for residents?
Tail coverage is an insurance policy that protects you against malpractice claims filed after you leave a position. It is a vital negotiation point because the "buy-out" cost can be substantial, sometimes reaching tens of thousands of dollars for surgical specialties. Securing an agreement where the employer assumes the cost of the tail ensures you aren't financially penalized when transitioning to future roles.
How do I know if a non-compete clause is reasonable in my specialty?
A reasonable non-compete typically limits its scope to a specific geographic radius, such as 5 to 10 miles, for a duration of 12 to 24 months. If the clause prevents you from practicing in an entire metropolitan area, it's likely overreaching. In 2026, you should verify how local regulations and recent federal shifts impact the enforceability of these restrictive covenants in your specific region.
Can I negotiate my schedule or call requirements as a new attending?
Yes, your clinical schedule and call frequency are often the most flexible parts of an employment agreement. You can negotiate for specific "post-call" days, a maximum cap on weekend shifts, or a gradual ramp-up period during your first year. Framing these requests as essential for clinical safety and long-term physician retention often makes them more acceptable to hospital leadership.
How does a physician contribution margin differ from a standard salary survey?
A salary survey only reflects what other doctors are paid, whereas a contribution margin quantifies the actual profit you generate for the healthcare system. This margin accounts for the difference between your total collections and the variable costs of your clinical work. Utilizing this metric during physician contract negotiation for residents allows you to justify your compensation through objective, system-level financial data.
Should I hire a lawyer to review my physician employment contract?
You should always engage a qualified healthcare attorney to review the legal language of your agreement. While economic platforms provide the data needed to negotiate your value, a lawyer identifies hidden risks in termination clauses and indemnification requirements. Combining economic clarity with legal expertise provides the most secure foundation for your transition from residency to attending status.


