

The 2026 CMS efficiency adjustment has finalized a 2.5% reduction in work relative value units for most surgical and diagnostic services, effectively penalizing physicians for the same clinical output. If you feel trapped in a wRVU-only model that fails to account for these regulatory shifts, you aren't alone. Many practitioners find that renegotiating physician employment contract terms feels like an uphill battle against hospital-controlled data and opaque benchmarks. It's easy to feel undervalued when the metrics used to measure your worth are fundamentally disconnected from the economic reality of your practice.
We understand the anxiety that comes with challenging institutional "black box" data, but there's a path toward transparency. This article will show you how to dismantle common negotiation myths by using objective economic data to secure a contract that reflects your true clinical value. We'll provide a clear framework for proving your economic impact, moving beyond simple productivity to look at contribution margins. By the end, you'll have the confidence to use external sources like CMS and RAND to ensure your compensation finally aligns with your actual contribution to the organization.
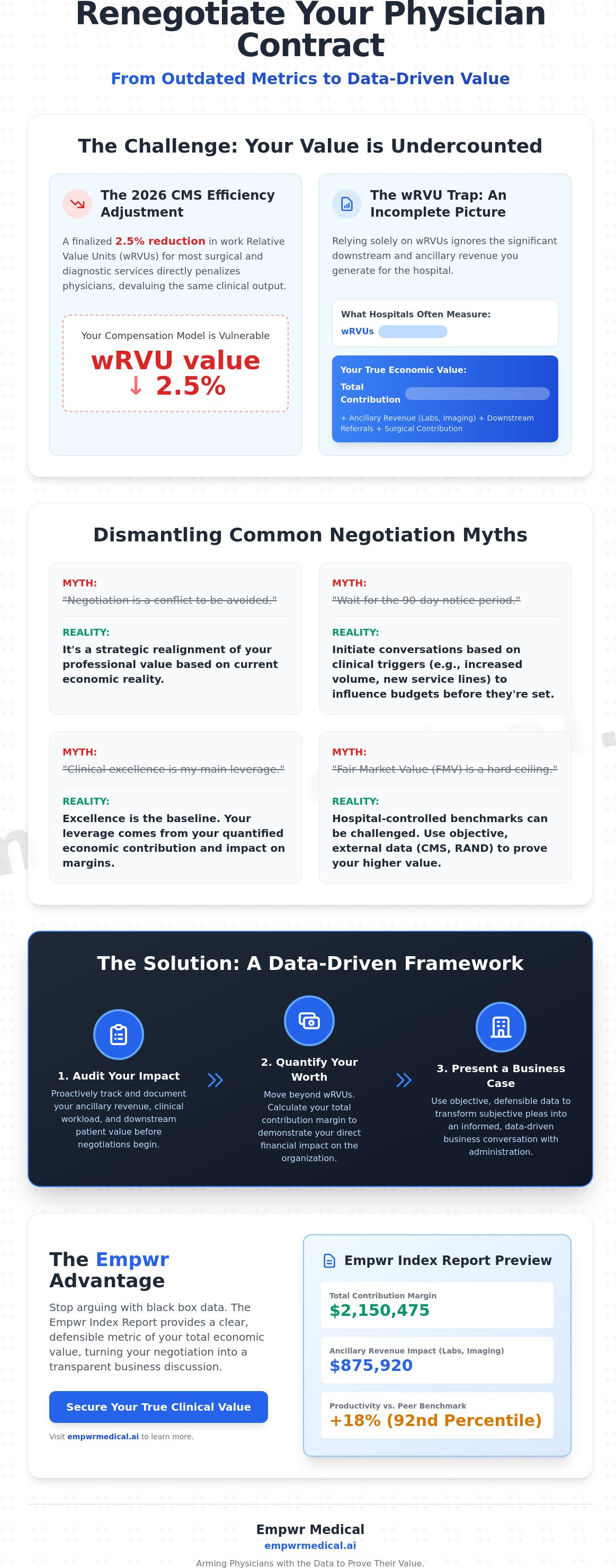
Key Takeaways
- View contract renegotiation as an ongoing strategic realignment of your professional value rather than a conflict reserved for the end of a term.
- Identify why wRVUs are an incomplete proxy for your financial worth, particularly as regulatory changes shift the valuation of clinical productivity.
- Challenge the "Fair Market Value" ceiling by utilizing objective data that captures your total contribution margin and ancillary revenue impact.
- Secure a stronger position when renegotiating physician employment contract terms by auditing your ancillary revenue and clinical workload before the meeting begins.
- Leverage the Empwr Index Report to provide a clear, defensible metric that transforms subjective pleas into an informed, data-driven business conversation.
Common Misconceptions When Renegotiating Physician Employment Contracts
Renegotiating physician employment contract terms is often viewed as a confrontational event, a high-stakes battle between a provider and an administrator. This perspective is fundamentally flawed. In 2026, successful renegotiation is a strategic realignment of value. It's the process of ensuring your compensation reflects the current economic reality of your practice. Many physicians hesitate to initiate these discussions because they feel like they're "asking for more" in a setting dedicated to patient care. However, the shift from 2025 to 2026 has brought a new standard of transparency. Hospitals are using sophisticated data to manage their margins. You must use the same level of rigor to manage your career. Applying established negotiation principles allows you to move past emotional appeals and toward a professional business conversation.
The landscape changed significantly between 2025 and 2026. With the 2.5% reduction in wRVU values for many surgical and diagnostic specialties, the old productivity-only arguments have lost their teeth. Administrators are now looking at total economic impact. If you don't bring your own data to the table, you're forced to accept their version of the truth. Transparency isn't just a buzzword; it's the only way to ensure a fair exchange of value in a consolidated healthcare market. It transforms a perceived conflict into a collaborative planning session.
The Timing Myth: When to Start the Conversation
A common mistake is waiting for the formal "90-day notice" period to begin discussions. By the time you reach this window, the hospital has likely already allocated its budget for the following year. Meaningful changes require a longer runway. You should monitor clinical triggers that alter your economic value in real-time. These include a sustained increase in patient volume, the launch of a new specialty service line, or a shift in the local payer mix. Strategic interruptions of automatic renewals are necessary when your contribution has outpaced the original contract's logic. If you wait for the expiration date, you've already lost your most significant window of influence.
The Leverage Myth: Why Clinical Excellence Isn’t Enough
Hospitals view clinical excellence as the baseline requirement for employment. Being a "good doctor" with high patient satisfaction scores is expected; it isn't leverage. To effectively navigate renegotiating physician employment contract specifics, you must distinguish between clinical quality and economic contribution. While your outcomes are vital for patient health, the hospital's administration focuses on contribution margins and downstream revenue. Data-driven advocacy is now the professional standard. You aren't just a clinician; you're an economic engine for the organization. Proving that engine's worth requires quantifying your impact beyond simple productivity metrics. Utilizing a Specialty-Specific Revenue Analysis allows you to show how your presence affects the hospital's bottom line through ancillary services and strategic growth.
The wRVU Trap: Why Your Clinical Productivity Isn’t Your Total Economic Value
For decades, the work Relative Value Unit (wRVU) has served as the default currency for physician productivity. While it offers a standardized way to measure volume, it fails spectacularly as a proxy for financial worth. Relying solely on wRVUs during the process of renegotiating physician employment contract terms ignores the actual revenue you generate for the healthcare system. The 2026 CMS efficiency adjustment, which reduced wRVUs for many procedural services by 2.5%, highlights the vulnerability of this metric. If your compensation is tied to a unit that can be devalued by regulatory fiat, your financial stability is at risk.
Hospitals often manipulate or stagnate conversion factors, claiming that "fair market value" restricts further increases. This narrative conveniently overlooks the "hidden" revenue streams your clinical decisions activate. Every laboratory order, imaging study, and surgical referral represents a line item on the hospital’s balance sheet that isn't captured in your wRVU count. To capture your full impact, you need a more comprehensive metric, such as a physician economic value score, which translates clinical effort into institutional profit. This shift in perspective is the difference between being viewed as a cost center and being recognized as a primary revenue driver.
Understanding the Contribution Margin Formula
The contribution margin is a fundamental financial metric that hospitals use internally but rarely share with providers. It is defined as your total generated revenue minus direct variable costs, such as medical supplies and clinical staff time. This figure reveals the actual profit you generate to cover the hospital's fixed overhead and executive salaries. Unlike wRVUs, which only track your time and effort, the contribution margin tracks your business impact. When you understand this formula, you stop arguing about how hard you work and start talking about how much you contribute. It provides a defensible basis for higher compensation that is grounded in the hospital’s own accounting logic.
Quantifying Downstream Revenue and System Impact
Downstream revenue includes every dollar that flows into the system because of your National Provider Identifier (NPI). This encompasses ancillary services and referrals to specialists within the same network. Integrated health systems place a high premium on "leakage prevention," which is the ability to keep patients within their ecosystem. If your practice patterns ensure that 90% of your referrals stay in-house, you're providing massive value that a standard productivity report will never show. Your value score must include these invisible revenue streams to be accurate. Transitioning from a volume-based mindset to a value-based one requires the right analytical tools. You can begin this process by requesting a Specialty-Specific Revenue Analysis to see the full scope of your economic footprint.
Debunking the "Fair Market Value" Standard in Hospital Negotiations
Administrators frequently use Fair Market Value (FMV) as a rigid ceiling during negotiations. They present survey data from organizations like MGMA as the final word on what you should earn. This creates a psychological barrier. It makes renegotiating physician employment contract terms feel like a request for an illegal exception rather than a market-based adjustment. The reality is that FMV is a range, not a fixed point. It's also based on data that is often flawed or incomplete. When a hospital claims they can't pay you more due to FMV constraints, they're often using a shield to protect their own margins.
Self-reported salary surveys rely on voluntary participation, which introduces significant bias. If you only look at these reports, you're seeing a filtered version of the market. To gain a true advantage, you must look at physician fair market value data derived from actual insurance claims and objective federal sources. This approach moves the conversation from what others say they make to what the services you provide are actually worth in the current economy. It transforms a subjective debate into a rigorous financial analysis.
The Flaw in Traditional Salary Surveys
Traditional surveys suffer from a persistent lag time, often reflecting data that is 12 to 18 months old. In the fast-moving economy of 2026, this delay effectively reduces your bargaining power. Participation bias also skews results, as large academic centers or specific practice types may be overrepresented. Most importantly, national averages fail to capture local market dynamics. They ignore the specific pricing power of your hospital system or the unique cost-of-living adjustments required in your specific geography. Relying on outdated averages is a recipe for stagnation.
Utilizing CMS and RAND Data for Objective Benchmarking
CMS fee schedules offer a transparent, real-time baseline for revenue. They don't rely on self-reporting; they reflect the actual government valuation of your clinical work. Additionally, data from the RAND Corporation provides deep insights into how private insurers pay hospitals relative to Medicare rates. If your hospital is collecting 300% of Medicare from private payers for your services but paying you based on the 50th percentile of a national survey, there's a massive disconnect. Using these objective sources allows you to counter "take it or leave it" offers with evidence that is difficult for administrators to dismiss.
Strategic Preparation: Moving Beyond Subjective Pleas to Objective Data
Many physicians believe they must hire a lawyer the moment they decide to start renegotiating physician employment contract terms. While legal counsel is vital for finalizing language, the initial phase of negotiation isn't a legal battle; it's a data audit. If you walk into a boardroom with a lawyer but no data, you've already ceded the economic high ground. Your preparation must begin with an objective audit of your clinical workload and the ancillary revenue tied to your NPI. This includes tracking every lab, imaging study, and referral you generate, which often remains invisible in standard productivity reports.
The second step involves comparing hospital-provided data against external clinical revenue analytics. Administrators often present "black box" data that minimizes your contribution margin. By utilizing the physician contract renewal negotiation framework, you can draft a value proposition that focuses on institutional health. This shifts the narrative from a personal request to a business case for the department’s success. When you present facts derived from independent sources, you force the administration to engage with your actual economic impact rather than their internal benchmarks. Access the Empwr Index Report to begin your data-driven audit today.
The Role of Specialty-Specific Revenue Analysis
A surgeon’s value is calculated differently than an internist’s because the billing structures are fundamentally distinct. A specialty specific revenue analysis accounts for unique billing codes and high-value technical components that general surveys miss. For proceduralists, tracking these technical components is essential. It proves that your presence in the OR generates revenue far beyond your professional fee. Without this specialty-specific lens, you're likely leaving significant money on the table because the hospital is capturing the technical fees while only paying you for the work units.
Choosing the Right Negotiation Software
In 2026, static spreadsheets are no longer sufficient for high-level negotiations. Modern software for physician contract negotiation provides real-time dashboards that allow for continuous value monitoring. These tools offer location-adjusted data, recognizing that a cardiologist in the Midwest, where average compensation is $400,000, faces different market pressures than one in the Northeast. Real-time data allows you to see how your value shifts as regional pricing and CMS schedules change. This level of clarity ensures that you're always negotiating from a position of strength, grounded in the most current economic realities.
Leveraging Data-Driven Insights for a Fairer Contract
Data serves as the ultimate equalizer in the often-unbalanced dynamic between physicians and hospital administrators. When renegotiating physician employment contract terms, you're usually operating with a significant information deficit. The hospital possesses the full picture of your billing, collections, and downstream impact, while you're often left with a simple productivity report. Bringing objective, external data to the table restores balance. It allows you to move from a position of defense to one of strategic alignment. You aren't just asking for a raise; you're presenting a business case for a fair market exchange.
A common myth suggests that data-driven negotiation damages the relationship with administration. In reality, the opposite is true. Professional administrators respect professional preparation. Moving away from subjective pleas and toward an "Informed Conversation" fosters professional respect. It signals that you understand the operational realities of the healthcare system. When you speak the language of contribution margins and economic value, you're no longer viewed as a cost center. You become a strategic partner in the organization's success.
The Empwr Index: Your Economic Value Score
The Empwr Index provides a single, defensible score that simplifies the complexities of your professional worth. Our methodology integrates CMS fee schedules, RAND hospital pricing data, and specialty-specific revenue nuances to create a high-level view of your impact. This isn't just another salary survey. It's a rigorous calculation of your true economic floor. By using a personalized report, you can ground the conversation in "hidden truths" that internal hospital data might obscure. This transparency provides the peace of mind that comes from knowing your contribution is quantified accurately. It translates complex backend financial processes into actionable results you can use at the bargaining table.
Next Steps for Your 2026 Renegotiation
Success in 2026 requires a proactive approach. You shouldn't wait until the month before your renewal to begin monitoring your value. The economic landscape is shifting too rapidly for reactive strategies. Start building your data trail today to ensure you're prepared for any clinical or regulatory triggers. For groups or departments looking to empower their entire team, enterprise licensing for our Physician Economic Value Platform offers a way to standardize fairness across the organization. It's time to move beyond the wRVU trap and secure a contract that reflects your actual contribution. You can quantify your value with Empwr Medical to ensure your next negotiation is grounded in reality rather than institutional myths.
Securing Your Professional Future Through Economic Clarity
The healthcare landscape of 2026 requires a departure from outdated productivity metrics and subjective bargaining. You've seen how the wRVU trap and stagnant "Fair Market Value" standards often obscure your true institutional worth. By shifting the focus toward contribution margins and objective external benchmarks, you transform renegotiating physician employment contract terms from a stressful conflict into an informed business conversation. This transition ensures your compensation reflects the actual revenue you generate through both direct care and ancillary system impact.
You deserve a strategy grounded in transparency and clinical precision. Empwr Medical is a physician-founded and led platform designed to bring hidden truths to light. Our methodology utilizes data sourced from CMS and RAND pricing benchmarks to provide specialty-specific and location-adjusted reporting that hospitals cannot ignore. You don't have to rely on opaque internal data or lagging salary surveys. Take the next step toward a fairer agreement and calculate your true economic value before your next negotiation. Your clinical excellence is the baseline; your economic impact is your leverage.
Frequently Asked Questions
When is the best time to start renegotiating a physician employment contract?
The ideal window to begin the process is six to 12 months before your current term expires. Waiting for the standard 90-day notice period is often too late because hospital budgets are typically finalized months in advance. Initiating the conversation early allows you to use clinical triggers, such as a sustained increase in patient volume or the launch of a new service line, as leverage for a strategic realignment of your value.
Can I renegotiate my contract if it has an evergreen or automatic renewal clause?
Yes, you can and should renegotiate despite an evergreen clause. These clauses are designed for administrative convenience, not to lock you into stagnant compensation. To interrupt the cycle, you must provide a formal request for amendment or a notice of non-renewal within the timeframe specified in your contract. This forces a discussion on how renegotiating physician employment contract terms can better reflect your current economic contribution to the health system.
What is the most important metric to use when asking for a salary increase?
Your contribution margin and downstream revenue impact are the most powerful metrics you can present. While wRVUs measure your clinical effort, the contribution margin reveals the actual profit you generate for the hospital after variable costs. Highlighting the revenue from labs, imaging, and surgical referrals tied to your NPI provides a defensible business case that goes far beyond simple productivity benchmarks.
How do I counter the hospital’s claim that I am already at the 75th percentile of MGMA?
Counter this claim by pointing out the inherent lag time and participation bias in traditional salary surveys. MGMA data often reflects market conditions from 12 to 18 months ago, failing to account for 2026 regulatory shifts like the 2.5% CMS wRVU reduction. Use objective, real-time data from CMS fee schedules and RAND pricing benchmarks to prove that your specific location and specialty-specific revenue generation justify a higher valuation.
Is it better to hire a lawyer or a consultant for physician contract renegotiation?
It's most effective to use both, but for different phases of the negotiation. A data-driven consultant or economic platform is essential during the preparation phase to establish your financial worth. Once you have agreed on the economic terms, a healthcare lawyer should review the final contract language. This ensures that legal protections, such as malpractice tail coverage and restrictive covenants, are properly structured.
What happens if the hospital refuses to share the data they used to calculate my bonus?
If an administrator refuses to provide transparency, you should treat it as a significant red flag for the relationship's long-term health. You can counter this "black box" approach by bringing your own independent Specialty-Specific Revenue Analysis to the table. Presenting your own data forces a reconciliation process where the hospital must either validate your numbers or explain why their internal metrics differ so significantly.
How does geographic location affect physician fair market value in 2026?
Geography remains a primary driver of compensation, with 2026 data showing average physician pay in the Midwest at $400,000, compared to $375,000 in the Northeast. Fair market value is not a national average; it's a local reality. Your negotiation strategy must account for regional payer concentrations, local competition for your specialty, and cost-of-living adjustments to ensure your contract remains competitive within your specific market.
Can residents and fellows renegotiate their initial employment offers?
Residents and fellows should absolutely negotiate, as over 70% of physicians who do so receive better terms. While you may lack a clinical track record at that specific institution, you can negotiate for higher signing bonuses, which in 2026 range from $10,000 for primary care to over $100,000 for certain surgical specialties. Focus on student loan repayment and relocation assistance as key areas where hospitals have significant flexibility for new recruits.


