

What if the exhaustion you feel at the end of a shift isn't just a result of patient volume, but a direct consequence of your economic invisibility? While the national burnout rate sits at 41.9% as of 2025, many clinicians find that the traditional wRVU treadmill fails to account for the true complexity of their work. You likely feel like a cog in a massive institutional machine, frustrated by a lack of transparency in how your salary is calculated. It's a heavy burden to carry when you suspect that physician burnout due to unfair compensation is the silent driver of your professional fatigue.
You deserve a professional environment where your value is translated into clear, objective data rather than abstract metrics. This article will show you how economic invisibility drives clinical exhaustion and how to leverage specialty-specific revenue analysis to reclaim your professional worth. We'll explore the direct link between financial fairness and mental health, then provide a methodical framework to help you quantify your impact. By the end, you'll be prepared for a data-driven negotiation that replaces contract renewal anxiety with quiet confidence.
Key Takeaways
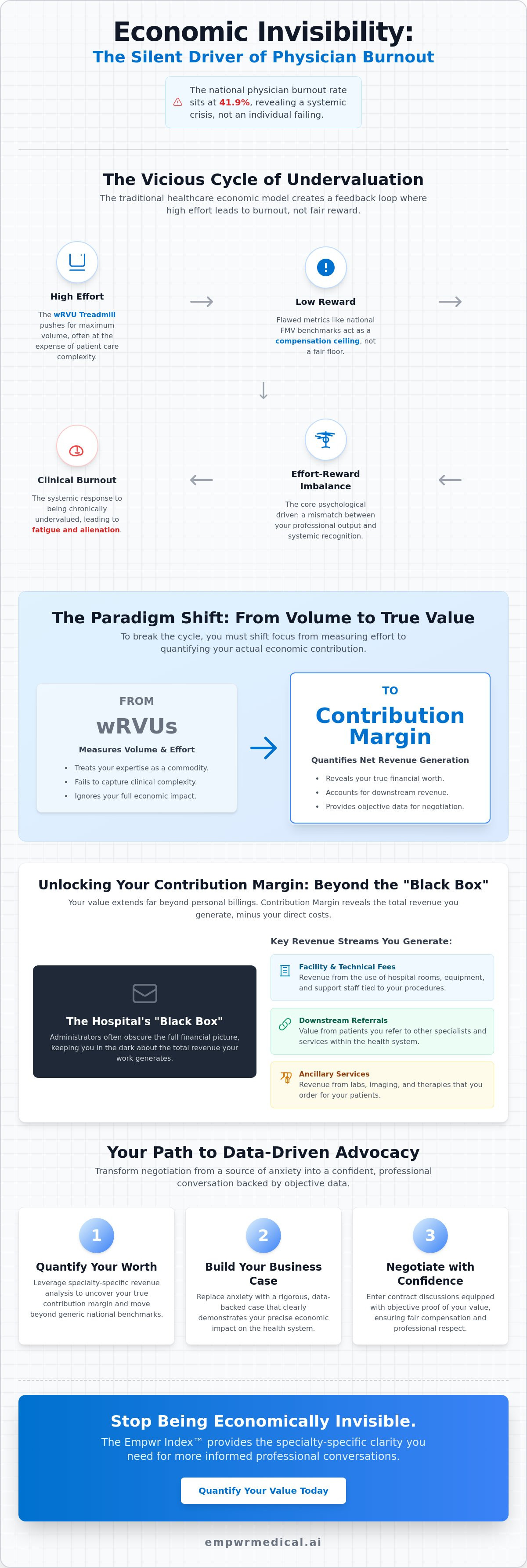
- Examine the Effort-Reward Imbalance (ERI) model to understand how clinical exhaustion is often a systemic response to undervalued professional contributions.
- Learn why national Fair Market Value benchmarks often serve as a compensation ceiling rather than a floor for your specific economic reality.
- Shift your perspective from volume-based wRVUs to your true Contribution Margin to accurately quantify the net revenue you generate for your system.
- Address the root causes of physician burnout due to unfair compensation by replacing negotiation anxiety with a rigorous, data-backed business case.
- Discover how the Empwr Index Report leverages specialty-specific revenue analysis to provide the clarity needed for more informed professional conversations.
The Link Between Compensation and Burnout: Beyond the wRVU Treadmill
For decades, the healthcare industry has treated Physician burnout as an individual psychological failing. This perspective is fundamentally flawed because it ignores the structural economic roots of clinical exhaustion. When the financial framework of a medical practice is misaligned with the actual value delivered, the resulting friction creates a unique type of distress. Specifically, physician burnout due to unfair compensation isn't merely about the number on a paycheck; it's about the erosion of professional respect and the systemic invisibility of your labor. You aren't just tired from seeing patients. You're exhausted from navigating a system that treats your specialized expertise as a commodity.
The traditional wRVU treadmill forces clinicians to work harder and faster while reimbursement rates often stagnate or decline. This creates a cycle where physicians are pushed toward maximum productivity without a proportional increase in professional or financial reward. Standard "resilience training" programs fail in these scenarios because they attempt to fix the physician rather than the broken economic structure. Asking a doctor to practice mindfulness while they're being squeezed by an inequitable contract is a form of institutional gaslighting. You can't breathe or meditate your way out of a compensation model that systematically undervalues your clinical output.
The Psychology of Effort-Reward Imbalance
Clinical exhaustion is frequently driven by the Effort-Reward Imbalance (ERI) model. This framework suggests that when high professional effort is paired with low rewards, whether financial or status-based, it triggers a chronic stress response. In medicine, this often manifests as moral injury. You're forced to prioritize volume over patient care to meet institutional quotas, creating a conflict between your ethical standards and your compensation structure. Effort-Reward Imbalance is the mismatch between professional output and systemic recognition. This imbalance signals to the physician that their contribution is not valued by the organization, leading to a profound sense of alienation and a decline in mental health.
Why Salary Surveys Alone Don’t Solve Burnout
Many health systems rely on broad national benchmarks like MGMA or Medscape to justify salary offers. These averages are often problematic because they ignore the specific economic impact an individual physician has on their local system. Broad benchmarks can suppress your leverage by treating your unique contributions as a generic data point. To have an informed conversation, you need physician fair market value data that is specialty-specific and adjusted for your actual clinical environment. Relying on generic data only deepens the sense of being a cog in a machine. True clarity requires moving beyond national medians to understand the granular financial reality of your specific practice and location.
Why Traditional Fair Market Value (FMV) Often Isn’t Fair
In the high-stakes environment of contract negotiations, health systems frequently present Fair Market Value (FMV) as an immovable legal barrier. They frame it as a regulatory ceiling that limits how much you can be paid without violating Stark Law or Anti-Kickback Statutes. However, this is often a strategic misinterpretation of the law. Administrators use FMV as a "ceiling" to cap earnings, rather than a "floor" that reflects your actual economic contribution. This creates a systemic environment where physician burnout due to unfair compensation thrives, as your professional value is artificially suppressed by institutional benchmarks that don't account for your specific clinical impact.
The "black box" of hospital accounting further complicates this issue. While you have clear visibility into your wRVU production, you're often kept in the dark regarding the facility fees, downstream referrals, and technical revenue your work generates. Without access to this data, you're negotiating in a vacuum. Reclaiming your professional standing requires quantifying physician value using independent data sources that bypass institutional gatekeepers. To gain this level of transparency, you can utilize a Physician Economic Value Platform to uncover the hidden financial truths behind your hospital's accounting.
The Limitations of Traditional Compensation Benchmarks
Standard salary surveys like MGMA or Medscape suffer from significant data lag. If you're negotiating a contract in 2026, the benchmarks presented to you likely rely on data collected in 2024. In an era of shifting Medicare conversion factors, such as the $33.4009 rate set for 2026, two-year-old data is functionally obsolete. Additionally, these surveys rely on voluntary participation, which introduces a selection bias that may not reflect the true market. Health systems use this aggregated, outdated data to justify lower-than-market offers, ignoring the individual nuances of your practice.
Accounting for Geographic and Specialty Nuances
Location and specialty play a critical role in your true economic worth. A cardiologist in a rural setting often carries a higher value than one in a saturated urban academic center because they may be the sole driver for an entire hospital service line. While CMS uses Geographic Practice Cost Indices (GPCI) to adjust reimbursements, many employment contracts fail to pass these adjustments through to the physician. You should seek a specialty specific revenue analysis to see exactly how your location and expertise translate into net revenue for your organization. Understanding these granular details is the only way to move from a position of exhaustion to one of informed advocacy.
Beyond wRVUs: Understanding Your True Contribution Margin
The prevailing compensation models in modern healthcare rely almost exclusively on the Work Relative Value Unit (wRVU). While this metric serves as a standardized way to measure physician activity, it is fundamentally a volume metric rather than a value metric. It tracks how many procedures you perform or patients you see, but it fails to capture the actual economic benefit those actions generate for the health system. When your worth is reduced to a single productivity number, the result is often physician burnout due to unfair compensation. You are pushed to work harder on a treadmill that doesn't account for the revenue you facilitate beyond your professional fees.
To move beyond this limited perspective, you must understand your Contribution Margin. This is the net revenue a physician brings to the system after direct expenses are subtracted. Hospitals often exclude facility fees and downstream revenue from physician compensation conversations, even though these are the primary drivers of institutional profit. By shifting from a productivity mindset to an economic value mindset, you can begin to translate your clinical efforts into quantifiable financial outcomes. This transition is essential for any clinician seeking to bridge the gap between institutional accounting and personal professional strategy.
Why wRVUs Fail to Capture Your Total System Impact
The wRVU model systematically ignores the essential non-clinical work that sustains a high-functioning medical department. Leadership roles, medical education, and quality improvement initiatives are often uncompensated or significantly undervalued in traditional contracts. This creates a direct correlation to clinical burnout, as physicians are forced to perform these "invisible" tasks on top of their clinical quotas. To better understand how these units are calculated and where the gaps lie, this physician relative value units explained guide provides the necessary data to decode your pay stub. Without this clarity, the wRVU treadmill continues to accelerate, leaving you with increasing stress and declining professional satisfaction.
The Importance of Contribution Margin in Valuation
Hospitals calculate your contribution margin by taking the total revenue you generate and subtracting direct variable costs, such as your salary, benefits, and clinical support staff. While administrators use these reports to make strategic decisions, they rarely share them with the physicians themselves. This lack of transparency keeps you in a weakened negotiating position. Your economic value is the sum of professional fees, facility fees, and strategic system growth. Accessing this data allows you to present a business case that reflects your true worth to the organization, rather than accepting a generic salary based on outdated averages.
From Exhaustion to Advocacy: Preparing for Data-Driven Negotiations
The transition from clinical exhaustion to professional advocacy begins when you stop viewing your salary as a subjective "request" and start viewing it as an objective business case. Most clinicians approach contract renewals from a defensive posture, focused on the fatigue caused by administrative burdens or the wRVU treadmill. However, addressing physician burnout due to unfair compensation requires you to dismantle the information asymmetry that exists between you and your administration. When you possess the same granular financial data that the hospital uses to measure its margins, your negotiation anxiety is replaced by the steady assurance of methodology.
Shifting your mindset is only the first step. You must also change your strategy. While many organizations suggest hiring legal counsel, a lawyer's effectiveness is limited by the quality of the data they are given to argue. By mastering physician contract negotiation through the lens of economic value, you move the conversation away from emotional appeals and toward a rigorous analysis of ROI. This empowers you to present yourself as a strategic asset whose retention is vital to the system's financial health. To begin this process, you can generate an Empwr Index Report to establish a baseline of your true market worth before entering the boardroom.
Auditing Your Clinical Revenue Potential
A comprehensive audit of your clinical impact involves more than just counting wRVUs. You must look at the specific CMS Medicare Physician Fee Schedule conversion factors, such as the $33.4009 rate set for 2026, and apply them to your unique procedural mix. By cross-referencing your volume with independent RAND pricing data, you can estimate the actual professional and facility revenue your practice generates. Tracking your payer mix—the ratio of private insurance to Medicare or Medicaid patients—is also essential for accurate modeling. Utilizing Empwr Index scores allows you to benchmark this potential against regional peers, ensuring your valuation is grounded in location-adjusted reality.
Framing Your Value Proposition to Leadership
Hospital administrators speak the language of margins, retention, and system growth. To be heard, you must translate your clinical efforts into these terms. Instead of focusing on the hours worked, highlight the downstream revenue and technical fees your presence facilitates. A powerful leverage point is the "cost of replacement." Between the average signing bonus of $38,000 and the lost revenue during a vacancy, replacing a productive physician represents a significant capital investment for any system. Using data to move the conversation from "I'm tired" to a demonstration of your $2M annual system impact changes the power dynamic of the negotiation entirely. This methodical approach ensures that your compensation reflects the full scope of your economic contribution.
Quantifying Your Worth with the Empwr Index™
Empwr Medical serves as a rigorous advocate for clinicians who refuse to accept the status quo of economic invisibility. Built by physicians for physicians, our Physician Economic Value Platform moves beyond the anecdotal to provide a definitive, data-backed assessment of your professional impact. By integrating authoritative data from CMS and the RAND Corporation, the platform ensures that every valuation is grounded in the same financial rigor used by institutional payers. This level of precision is the most effective countermeasure against physician burnout due to unfair compensation, as it replaces systemic ambiguity with objective evidence.
The centerpiece of this methodology is the Empwr Index, a single, clear score that represents your total economic value. Unlike generic calculators, our platform utilizes specialty-specific workflows to ensure that the unique economic drivers of different fields are respected. A neurosurgeon's value, heavily influenced by complex facility fees and high-acuity downstream revenue, is calculated using a different model than a pediatrician's value, which might focus more on population health and preventative system growth. This granular approach ensures that every clinician, regardless of their specialty, receives a valuation that reflects their true contribution to the health system.
Translating Clinical Workload into Clear Revenue Estimates
The platform performs a complex translation of your clinical workload, moving from raw CPT codes to specific dollar amounts. This process accounts for the nuances of different healthcare delivery models, ensuring that your estimates are accurate for your specific employment context. Location-adjusted data is central to this calculation. Because the economic reality of a practice in a rural setting differs significantly from one in an urban academic center, our models utilize regional benchmarks to ensure your market worth is contextual. This transparency allows you to see the technical and facility revenue that is typically hidden behind institutional accounting walls.
Using the Empwr Index to Drive Informed Conversations
An Empwr Index Report is more than a data point; it is a physical asset designed to be used during high-stakes contract renewals. Presenting a third-party, specialty-specific revenue analysis changes the power dynamic of the meeting, moving the discussion from a request for a raise to an informed conversation about system ROI. Because markets shift rapidly, an annual subscription ensures your valuation data remains current as Medicare conversion factors and regional benchmarks evolve. You can see how the Empwr Index can transform your next contract negotiation by providing the clarity needed to reclaim your professional value and mitigate the economic roots of exhaustion.
Reclaiming Your Professional Value Through Economic Clarity
Addressing the systemic roots of clinical exhaustion requires a fundamental shift from volume-based metrics to a comprehensive understanding of your contribution margin. By moving beyond the wRVU treadmill and outdated national benchmarks, you can dismantle the information asymmetry that often drives physician burnout due to unfair compensation. This transition from being a "cog in the machine" to a data-driven advocate is essential for your long-term career sustainability and well-being. It's time to replace institutional ambiguity with the steady assurance of objective evidence.
Empwr Medical provides the rigorous methodology needed for this transformation. As a physician-founded and led platform, we utilize authoritative CMS and RAND data sources to deliver specialty-specific and location-adjusted reporting. This level of precision ensures your valuation is grounded in reality rather than administrative convenience. You've already mastered the complexities of clinical care; now you can master the economic data that defines your professional worth.
Calculate your true economic value and start your informed conversation today. You deserve a professional future defined by clarity and mutual respect.
Frequently Asked Questions
Can unfair compensation alone cause physician burnout?
While burnout is a multifactorial phenomenon, unfair compensation is a primary systemic driver because it signals a lack of professional respect and institutional invisibility. When clinical effort is not met with equitable financial reward, it leads to moral injury and a sense of alienation. This specific type of physician burnout due to unfair compensation is often resistant to standard resilience training because the underlying cause is a broken economic structure rather than a lack of individual stress management.
What is the "Effort-Reward Imbalance" in healthcare?
The Effort-Reward Imbalance (ERI) is a psychological model where high professional output is paired with low rewards, triggering chronic stress and clinical exhaustion. In a medical context, this occurs when physicians are pushed toward maximum productivity on a wRVU treadmill without a proportional increase in recognition or financial stability. This imbalance tells the clinician that their specialized expertise is viewed as a commodity, which is a significant predictor of long-term professional dissatisfaction.
How do I know if I am being paid fairly compared to my peers?
Determining fairness requires moving beyond national medians to analyze location-adjusted and specialty-specific data. You must evaluate your total economic impact, including facility fees and downstream revenue, rather than just your base salary. If your compensation doesn't reflect the current 2026 Medicare conversion factor of $33.4009 or regional cost indices, you may be undervalued. Utilizing a specialty-specific revenue analysis provides the necessary clarity to benchmark your worth against the actual market.
What is a "Contribution Margin" and why should a doctor care?
Contribution margin is the net revenue a physician generates for a health system after direct variable expenses, such as salary and clinical support, are subtracted. Doctors should care because this metric captures the technical and facility fees that are typically omitted from standard pay stubs. Understanding your contribution margin allows you to see the full profit you bring to the organization. This data is essential for addressing physician burnout due to unfair compensation by uncovering your true system-wide value.
Why are wRVUs considered a poor measure of a physician’s true value?
wRVUs are a measure of clinical volume and activity, not the actual economic value or strategic growth you facilitate. They ignore critical non-clinical contributions like leadership, medical education, and quality improvement initiatives that sustain a high-functioning department. Because wRVUs are decoupled from the actual revenue generated by procedures and facility fees, they provide an incomplete picture of your worth. Relying solely on this volume metric forces clinicians into a productivity cycle that ignores their broader impact.
Can I negotiate my contract if I am part of a large health system?
Negotiation is entirely possible within large systems, provided you replace emotional appeals with a rigorous, data-driven business case. Administrators respond to objective metrics such as return on investment (ROI), the high cost of physician replacement, and specialized market scarcity. When you present an independent valuation of your system impact, you shift the power dynamic from a request for a raise to a strategic conversation. Clarity and objective data are your most effective tools for navigating institutional bureaucracy.
What data sources are most reliable for physician salary benchmarks?
The most reliable benchmarks are derived from authoritative, primary sources like the CMS Medicare Physician Fee Schedule and independent RAND pricing data. These sources provide a more accurate and timely reflection of the market than voluntary surveys, which often suffer from significant data lag. Using current 2026 regulatory standards ensures that your valuation is grounded in the same financial reality used by payers. This methodical approach provides the steady assurance needed for high-level professional strategy.
How does the Empwr Index differ from a standard salary calculator?
The Empwr Index is a comprehensive valuation platform that translates CPT codes and clinical workflows into a single, clear score of economic value. Unlike a generic calculator that uses broad averages, it accounts for geographic nuances and specialty-specific revenue drivers. It provides a detailed Empwr Index Report that captures facility fees and downstream impact, offering a level of transparency that standard tools cannot match. This platform acts as a bridge between dense institutional data and your personal negotiation strategy.


